antibacterial and antiviral prescribing following bite wounds
Last edited 07/2021 and last reviewed 11/2023
- antibacterial prophylaxis:
- prophylactic antibacterial therapy should be offered to patients who:
- sustain bites to the hand, or from humans or cats
- antibacterial prophylaxis is a reasonable precaution when the wound involves moderate or severe injury, or crush or puncture injury; when oedema is present; when bone or joint penetration is possible; when a bite injury to the face has been closed; when the genital area is involved; for complicated dog bites (e.g. those requiring surgical debridement); for patients who are immunosuppressed, have diabetes or prosthetic heart valves; or where the injury is near a prosthetic joint (1)
- PHE guidance states (2):
- human bite
- assess risk of tetanus, HIV, hepatitis B&C
- antibiotic prophylaxis is advised
- animal bite
- assess risk of tetanus and rabies
- give antibiotic prophylaxis if cat bite/puncture wound;
bite to hand, foot, face, joint, tendon, ligament; immunocompromised/diabetic/asplenic/cirrhotic/
presence of prosthetic valve or prosthetic joint
- human bite
- which antibiotic:
- co-amoxiclav (625mg three times daily for adults) is the antibacterial
of choice for initial prophylaxis, or the treatment of established
infection, before culture and sensitivity results are available
- if penicillin allergic (2):
- metronidazole PLUS doxycycline (cat/dog/man) or
- metronidazole PLUS clarithromycin (human bite)
- review at 24 and 48 hours (2) - because the recommended
regimen covers the majority, but not all, of the likely pathogens
from an animal or human bite
- if penicillin allergic (2):
- co-amoxiclav (625mg three times daily for adults) is the antibacterial
of choice for initial prophylaxis, or the treatment of established
infection, before culture and sensitivity results are available
- prophylactic antibacterial therapy should be offered to patients who:
- antiviral prophylaxis:
- human bites
- a risk assessment should be made and, where appropriate, hepatitis B vaccine and/or specific hepatitis B immunoglobulin and/or HIV post-exposure prophylaxis should be offered
- there is no post-exposure prophylaxis for hepatitis C, which appears to be transmitted more easily than HIV. However, a patient exposed to hepatitis C will need sequential tests for seroconversion, and appropriate referral
- human bites
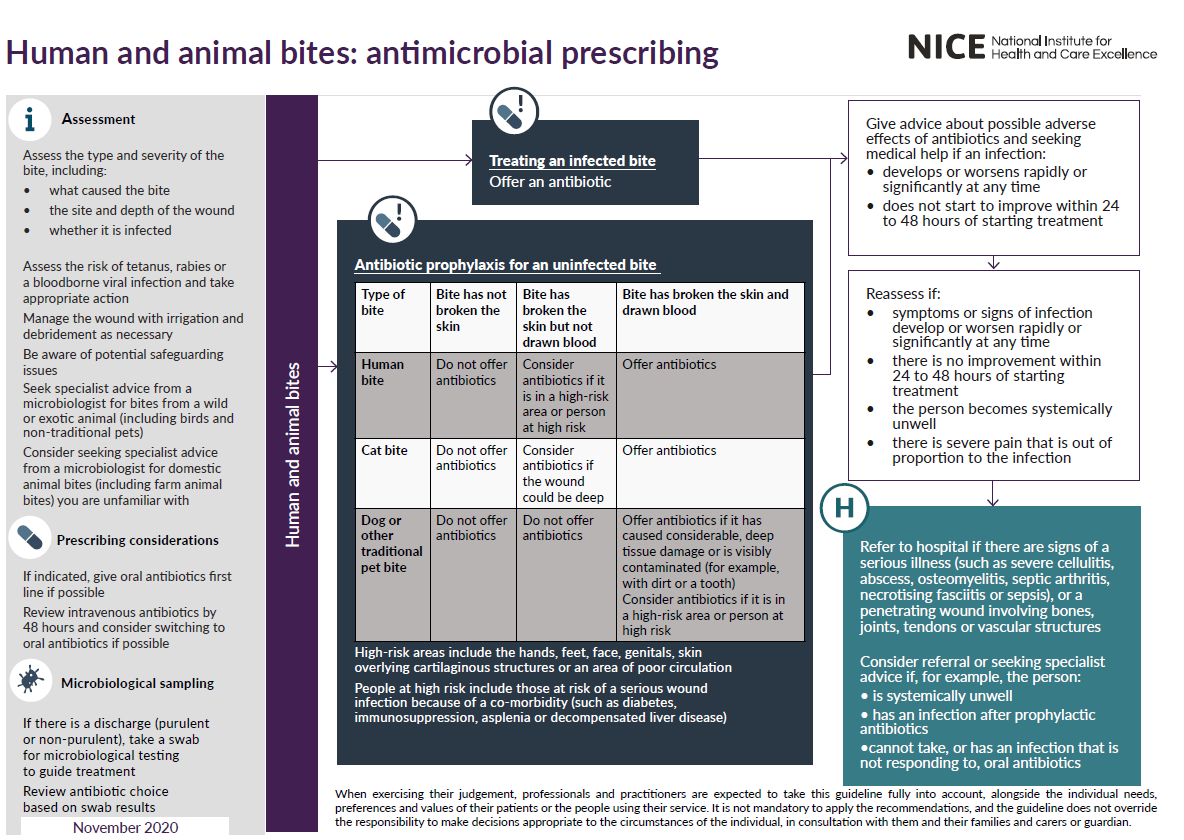
NICE have suggested a schemata for managing human and anima bites (3):


Reference: