assessment of vaginal discharge
Last edited 05/2019 and last reviewed 03/2022
Various aspects of the history may be SUGGESTIVE of particular infectious causes of an increased vaginal discharge.
- pregnancy, diabetes mellitus, recent antibiotic treatment, immunosuppression, dyspareunia or itchy vulval irritation - suggestive of candidiasis
- a recent change in sexual partner, a discharge that is offensive and copious - suggestive of trichomoniasis
- offensive discharge plus IUCD plus dyspareunia - sugggestive of bacterial vaginosis
- erythema and oedema of the vulvovaginal area, excoriation of the vulva and presence of curd-like discharge with white plaques - suggestive of candidiasis
- yellow/green, offensive, frothy discharge - suggestive of trichonomiasis
- bacterial vaginosis is suggested by a thin, offensive, grey-white, adherent discharge
Management of Women Presenting with Vaginal Discharge outside the Genitourinary Medicine Clinic Setting (1)
- Clinical and sexual history
- when a woman presents with a vaginal discharge that she feels is different
from her normal discharge this should be assessed by first taking a clinical
history
- she may have underlying concerns (e.g. STI or cancer) or specific expectations that should be explored
- the presence of vaginal discharge is, in itself, a poor predictor of
an STI
- nevertheless, a sexual history (e.g. number and gender of partners,
sexual activities, use of condoms) should be taken to assess the risk
of STIs
- sexually active women are at higher risk of STI if they are
- aged <25 years; or
- have changed their sexual partner or
- had more than one sexual partner in the last 12 months
- sexually active women are at higher risk of STI if they are
- other risk factors include a lack of consistent condom use, and a previous diagnosis of chlamydia infection in the last 12 months
- nevertheless, a sexual history (e.g. number and gender of partners,
sexual activities, use of condoms) should be taken to assess the risk
of STIs
- when a woman presents with a vaginal discharge that she feels is different
from her normal discharge this should be assessed by first taking a clinical
history
Assessment of symptoms
- symptoms associated with vaginal discharge can guide a health professional
to the most likely cause
Sign/Symptom Bacterial Vaginosis Candida Trichomoniasis Discharge Thin Thin White Scanty to profuse Odour Offensive/fishy Non-offensive Offensive Itch none vulval itch vulval itch Other possible symptoms Soreness; Dysuria;Superficial dyspareunia
Dysuria; lower abdominal pain Visible signs Discharge coating the vagina and vestibule;
No vulval inflammation
Normal findings OR
Vulval erythema; Oedema; fissuring; satellite lesions
Frothy yellow discharge; vulvitis; vaginitis; cervicitis; 'Strawberry cervix' (ectocervix sometimes resembles the surface of a strawberry) Point-of-care test: vaginal pH > 4.5 pH <= 4.5 >4.5 - the characteristics of the vaginal discharge should be determined:
- what has changed
- onset
- duration
- odour
- cyclical changes
- colour
- consistency
- cxacerbating factors (e.g. after intercourse)
- enquiry should also cover any associated symptoms:
- itching a
- superficial dyspareunia a
- vulval or vaginal pain
- dysuria
- abnormal bleeding (heavy, intermenstrual or postcoital) b
- deep dyspareunia b
- pelvic or abdominal pain b
- fever b
NB.
- a - itching or superficial dyspareunia may indicate dermatological disease (e.g. lichen planus), which can be associated with vaginal discharge
- b - these symptoms are indicative of upper genital tract infection
Examination, point-of-care investigations and STI testing
- history-taking alone may guide health professionals towards the most likely
diagnosis but diagnostic accuracy varies
- in addition to the clinical and sexual history, physical examination and vaginal pH may be helpful
- should be standard clinical practice to offer to examine people presenting
with genital symptoms
- howeve if the history indicates candidiasis or BV, the risk of
STI is low, and there are no symptoms indicative of upper genital
tract infection, treatment for candidiasis or BV may be given without
examination (i.e. syndromic management)
- women should be advised to undergo examination if symptoms persist
or reoccur
Schemata for diagnosis of Candida, BV and TV by signs and symptoms in adult women (2)
- women should be advised to undergo examination if symptoms persist
or reoccur
- howeve if the history indicates candidiasis or BV, the risk of
STI is low, and there are no symptoms indicative of upper genital
tract infection, treatment for candidiasis or BV may be given without
examination (i.e. syndromic management)
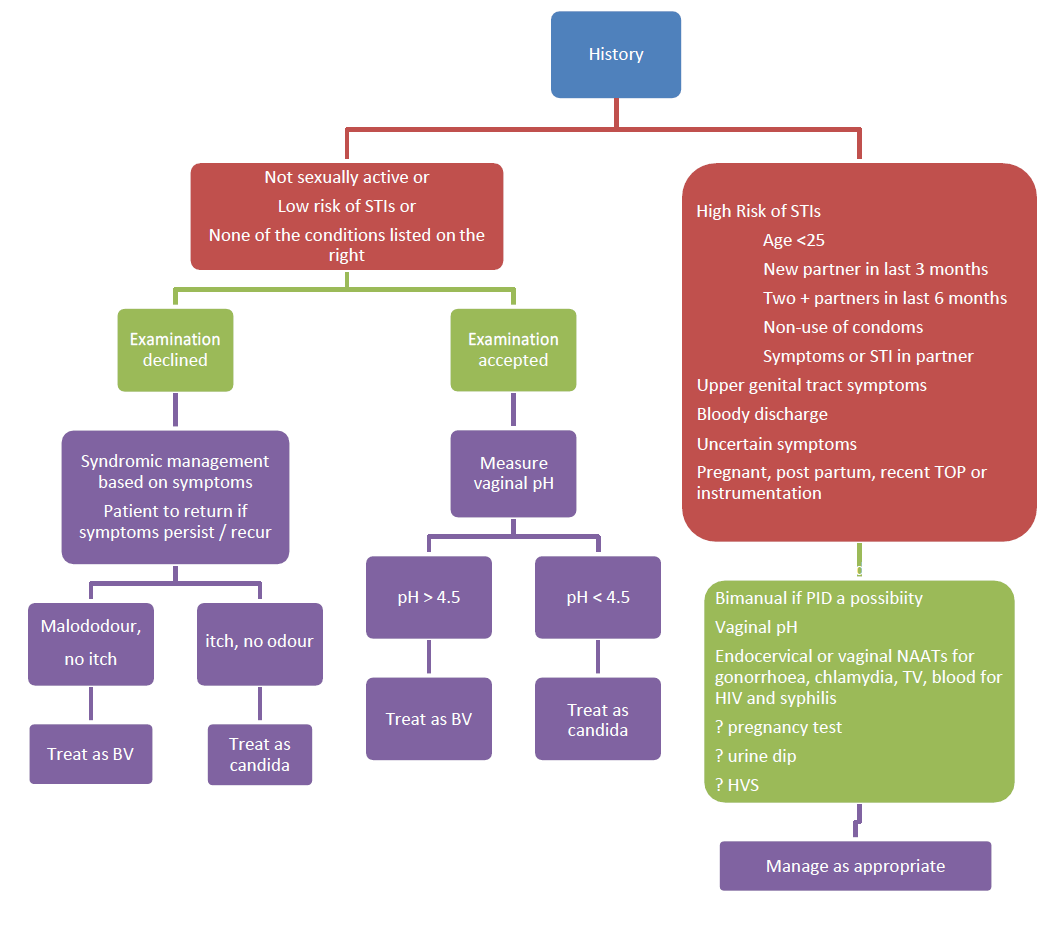
- STI testing should ideally be offered to all sexually active women
- for women who decline an offer of examination, a self-taken vulvovaginal swab (VVS) may be an option for chlamydia +/-gonorrhoea testing by nucleic acid amplification test (NAAT)
- urine tests are appropriate for men but in women NAAT testing of VVS or endocervical swabs are preferable to urine
- women who accept examination should have a vaginal pH measurement
using narrow range pH paper (pH 4-7)
- secretions should be collected from the lateral sides of the vaginal wall using a loop or swab. Vaginal pH testing can be used to assess the likelihood of candida (pH<= 4.5) or of BV or TV (pH >4.5) but it cannot distinguish between BV and TV
- if STI testing is indicated and/or requested, endocervical swabs
for chlamydia and gonorrhoea should also be taken, and a high
vaginal swab (HVS) may be indicated in some cases
- physical examination should include:
- inspection of the vulva (for obvious discharge, vulvitis, ulcers, other lesions or changes)
- speculum examination (inspection of: vaginal walls, cervix, foreign bodies; amount, consistency and colour of discharge)
- where there is any suggestion of upper genital tract infection physical
examination should also include:
- abdominal palpation (for tenderness/mass)
- bimanual pelvic examination (adnexal and/or uterine tenderness/mass, cervical motion tenderness)
- there is agreement in the UK that the minimum tests that constitute
an STI screen are chlamydia, gonorrhoea, syphilis and HIV tests
- lengthy pre-test discussion is not required unless a patient needs or requests this
- HIV testing in primary care settings has been encouraged by Chief Medical and Nursing Officers
Reference:
- 1) FSRH and BASHH Guidance (February 2012) Management of Vaginal Discharge in Non-Genitourinary Medicine Settings.
- 2) Oxfordshire Clinical Commissioning Group. Investigation and Management of Vaginal Discharge in Adult Women (Accessed 23/5/19)
nucleic acid amplification tests (NAATs) in investigation of vaginal discharge