spirometry in diagnosis of COPD
Last edited 02/2021 and last reviewed 07/2021
- Think of diagnosis of COPD in patients who are (1,2):
- over 35 and
- smokers or ex-smokers and
- have any of these symptoms:
- exertional breathlessness
- chronic cough
- regular sputum production
- frequent winter ’bronchitis’
- wheeze
- and have no clinical features of asthma , for example in asthma
(1):
- commonly develops symptoms under age 35 years old
- chronic productive cough is uncommon
- beathlessness is variable
- night-time waking with breathlessness and/or wheeze is common
- significant diurnal or day-to-day variability of symptoms is common
- other factors to consider include (3):
- recurrent lower respiratory tract infection
- history of risk factors
- host factors – genetic factors, congenital/developmental abnormailities
- tobacco smoke
- smoke from home cooking and heating fuel
- occupational dust, vapors, fumes, gases and other chemicals
- family history of COPD and/or childhood factors
- e.g. – low birthweight, childhood respiratory infections
etc(1).
- e.g. – low birthweight, childhood respiratory infections
etc(1).
- When thinking about a diagnosis of COPD, ask the person if they have:
- weight loss
- reduced exercise tolerance
- waking at night with breathlessness
- ankle swelling
- fatigue
- occupational hazards
- chest pain
- haemoptysis
- these last 2 symptoms are uncommon in COPD and raise the possibility
of alternative diagnoses
- one of the primary symptoms of COPD is breathlessness
- the Medical Research Council (MRC) dyspnoea scale (see linked item) should be used to grade the breathlessness according to the level of exertion required to elicit it
If COPD seems likely then perform post bronchodilator spirometry to confirm the diagnosis (2):
- presence of a post bronchodilatory FEV1/FVC < 0.7 confirms persistence airflow limitation and thus a diagnosis of COPD in patients with appropriate history and symptoms
- consider alternative diagnoses or investigations in:
- older people without typical symptoms of COPD where the FEV1/FVC ratio is < 0.7
- younger people with symptoms of COPD where the FEV1/FVC ratio
is ≥ 0.7
- in most patients routine spirometric reversibility testing is not necessary as a part of the diagnostic process or to plan initial therapy with bronchodilators or corticosteroids. It may be unhelpful or misleading because:
- repeated FEV1 measurements can show small spontaneous fluctuations
- the results of a reversibility test performed on different occasions can be inconsistent and not reproducible
- over-reliance on a single reversibility test may be misleading unless
the change in FEV1 is greater than 400 ml
- asthma may be present if:
- there is a large ( > 400 ml) response to bronchodilators
- serial peak flow measurements show significant diurnal or day-to-day variability
- there is a large ( > 400 ml) response to 30 mg prednisolone daily for 2 weeks
- asthma may be present if:
- the definition of the magnitude of a significant change is purely arbitrary
- response to long-term therapy is not predicted by acute reversibility testing (2,3)
If COPD seems likely then perform post bronchodilator spirometry to confirm the diagnosis (1):
- identifying airflow obstruction in COPD patients is critical in making the diagnosis
- airflow
obstruction is defined as (1):
- FEV1 < 80% predicted
- and FEV1/FVC < 0.7
- if still doubt about diagnosis consider the following
pointers (1) :
- clinically significant COPD is not present if FEV1 and FEV1/FVC ratio return to normal with drug therapy
- asthma may be present
if:
- there is a large ( > 400 ml) response to bronchodilators
- serial peak flow measurements show significant diurnal or day-to-day variability
- there is a large ( > 400 ml) response to 30 mg prednisolone daily for 2 weeks
- airflow
obstruction is defined as (1):
Notes:
- identifying early disease
- perform spirometry in people who are over 35, current or ex-smokers, and have a chronic cough
- consider spirometry in people with chronic bronchitis. A significant
proportion of these people will go on to develop airflow limitation
- NICE suggest that post-bronchodilator spirometry should be measured to confirm the diagnosis of COPD (2). The use of post-bronchilator spirometry is used in the updated classification of COPD (2):
- Assessment and classification of severity of airflow obstruction
The severity of airflow obstruction should be assessed according to the reduction in FEV1 as shown in table
Post-bronchodilator FEV1/FVC FEV1 % predicted Severity of airflow obstruction
Using NICE clinical guideline 12 (2004)
Severity of airflow obstruction
Using ATS/ERS 2004
Severity of airflow obstruction
Using GOLD 2021
Severity of airflow obstruction
Using NICE clinical guideline 101 (2010)
Post-bronchodilator Post-bronchodilator Post-bronchodilator < 0.7 >80% Mild Stage 1 - Mild Stage Stage 1 - Mild* < 0.7 50-79% Mild Moderate Stage 2 - Moderate Stage 2 - Moderate < 0.7 30-49% Moderate Severe Stage 3 - Severe Stage 3 - Severe < 0.7 < 30% Severe Very severe Stage 4 - Very severe Stage 4 - Very severe ** *Symptoms should be present to diagnose COPD in people with mild airflow obstruction
**Or FEV1 < 50% with respiratory failure.
GOLD guidance categories patients based on Symptoms via the ABCD categories:
The refined ABCD assessment tool (3)
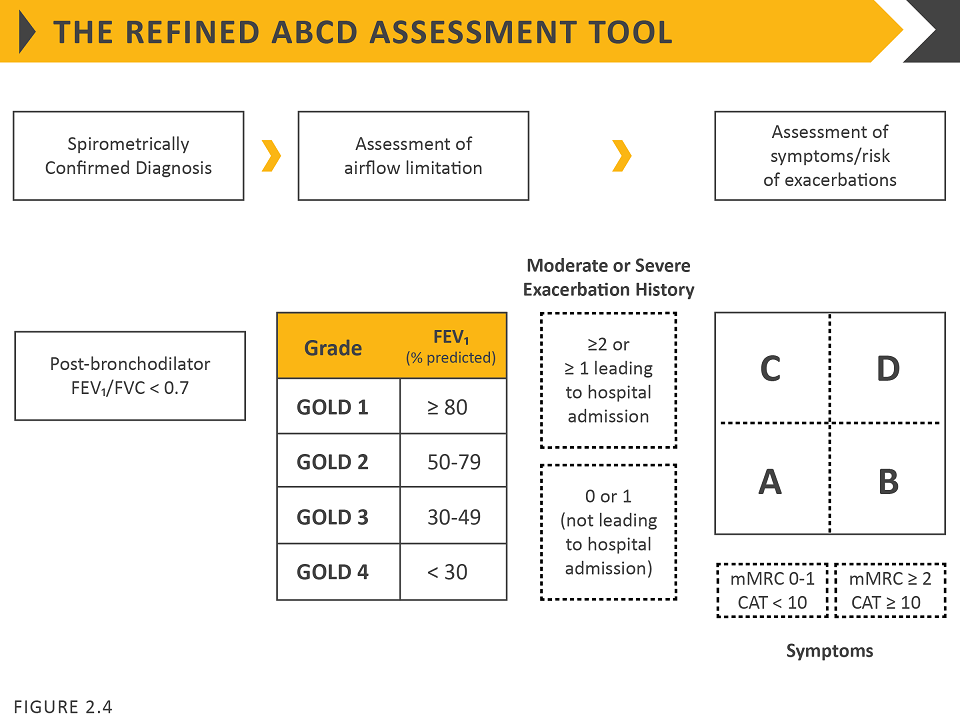
The categories are therefore defined via consideration of two specific features:
- exacerbation history and
- symptom Score (either assessment of dyspnoea via mMRC OR assessment of symptoms via CAT)
Category A is defined by:
Moderate or Severe Exacerbation History Symptom Score 0 or 1 (not leading to hospital admission) mMRC 0 or 1 or CAT <10
Category B is defined by:
Moderate or Severe Exacerbation History Symptom Score 0 or 1 (not leading to hospital admission) mMRC >=2 or CAT >=10
Category C is defined by:
Moderate or Severe Exacerbation History Symptom Score >=2 or 1 leading to hospital admission mMRC 0 or 1 or CAT <10
Category D is defined by:
Moderate or Severe Exacerbation History Symptom Score >=2 or 1 leading to hospital admission mMRC >=2 or CAT >=10
The combined COPD assessment allows patients with the same FEV1 (defined by the GOLD criteria) to be differentiated based on symptomatology, for example
- a subject with an FEV1 <30% with an mMRC of 2 and three exacerbations in the past year would be labelled GOLD grade 4, group D;
- wheres a subject with an FEV1 < 30% with an mMRC of 1 and zero exacerbations in the past year would be labelled GOLD grade 4, group A
Reference:
- (1) NICE (February 2004). Chronic obstructive pulmonary disease - management of chronic obstructive pulmonary disease in adults in primary and secondary care.
- (2) NICE (December 2018). Chronic obstructive pulmonary disease
- (3) Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2021. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease
chronic obstructive airways disease (COPD)
BODE index (BMI , airflow obstruction , dyspnoea and exercise capacity)
distinguishing asthma and COPD
intrathoracic and extrathoracic causes of cough when considering a diagnosis of COPD
Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria