when contraception can be stopped
Last edited 02/2020
Menopause is usually a clinical diagnosis made retrospectively after 1 year of amenorrhoea (1)
- most women do not require measurement of their serum hormone levels to make the diagnosis (1)
If not using hormonal contraception then:
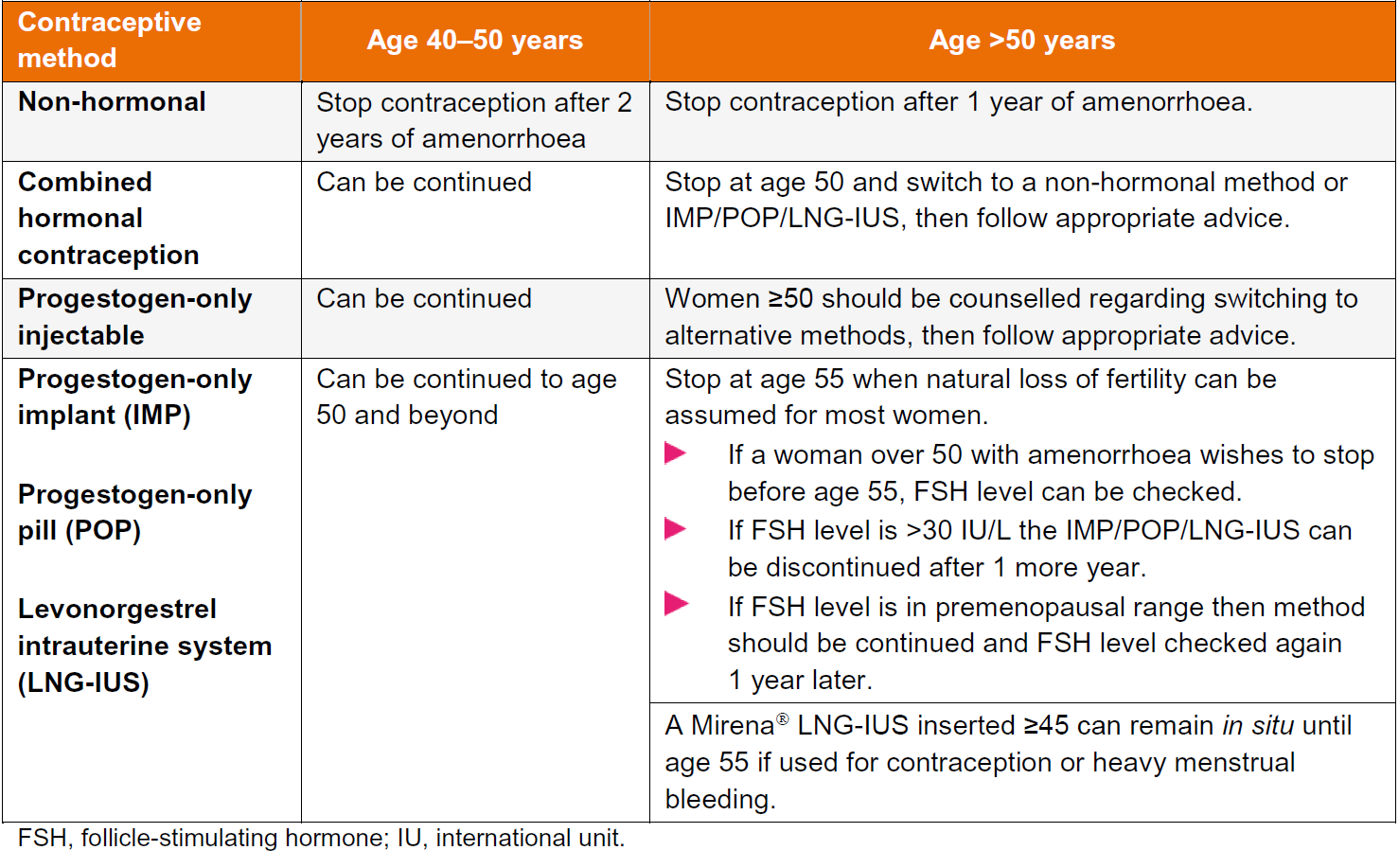
- if under 50 years can stop contraception after two years amenorrhoea (1,2,3,4)
If using contraception:
- if needed, women over 50 using progestogen-only contraception, including DMPA, can have serum follicle-stimulating hormone (FSH) measurements undertaken to check menopausal status
- the post-menopause is characterised by low levels of serum estradiol and raised levels of FSH and LH. As a general guide, a serum FSH level >30 IU/L indicates a degree of ovarian insufficiency, but not necessarily sterility (4)
- during perimenopause, isolated serum estradiol, FSH and LH levels can be misleading and should not be used as a basis for providing advice about stopping contraception; ovulation may still occur with risk of pregnancy, particularly in young women with a diagnosis of premature ovarian insufficiency.For this reason, the FSRH suggests restricting measurement of serum FSH for advice about stopping contraception to women over 50 using POC (non-injectable progestogen-only contraception) who are amenorrhoeic (4)
- women using CHC (combined hormonal contraception) or HRT (hormone replacement therapy) have suppressed levels of estradiol and gonadotrophins (FSH/LH)
- measuring these hormones does not give accurate information on which to base advice regarding menopausal status and when to stop contraception
- if using COC - can be prescribed in low-risk women until aged 50
years
- at aged 50 years switch to an alternative method of contraception. Subsequently follow advice on stopping contraception as per method used
- in general, all women can cease contraception at age 55 as spontaneous conception after this age is exceptionally rare even in women still experiencing menstrual bleeding
- if a woman aged 55 or over does not wish to stop a particular method, consideration can be given to continuation providing the benefits and risks for her as an individual have been assessed and discussed with her (4)
- IUC should not be left in situ indefinitely after it is no longer required as it could become a focus of infection.
Recommendations regarding stopping contraception
Notes:
- after counselling (about declining fertility, risks associated with insertion,
and contraceptive efficacy), women who have a Cu-IUD containing >=300 mm2
copper, inserted at or over the age of 40 years, can retain the device until
the menopause or until contraception is no longer required
- women who continue to use their IUD until contraception is no longer required should be advised to return to have the device removed
- if a woman is using DMPA and has elevated FSH levels, HCPs can be confident that the increased levels are due to perimenopause
- DMPA can suppress FSH to some extent which means a woman using DMPA could be menopausal yet show no increase in FSH levels. The optimum time to measure FSH levels in a woman using DMPA is just before a repeat DMPA is administered
- the Mirena can remain in situ for contraception until menopause if inserted at or after the age of 45
Reference:
- Prescribers’ Journal 2000;40 (2):121-129.
- Pulse September 17th 2005: 62-4
- FSRH (2010). Contraception for Women Aged Over 40 Years.
- FSRH (2019). Contraception for Women Aged Over 40 Years.