diagnosis
Last edited 11/2019
HFpEF diagnosis:
- The American Heart Association (1) and European Society of cardiology (2) are broadly in agreement with their definitions of HFpEF as representing patients with signs and symptoms of heart failure, evidence of normal or preserved ejection fraction but objective evidence of other structural or functional alterations in cardiac structure
- ESC guidelines are more descriptive in terms of specifying particular markers of diastolic dysfunction and also taking into account stress testing, although both emphasize the importance of ruling out noncardiac causes of symptoms.
AHA criteria:
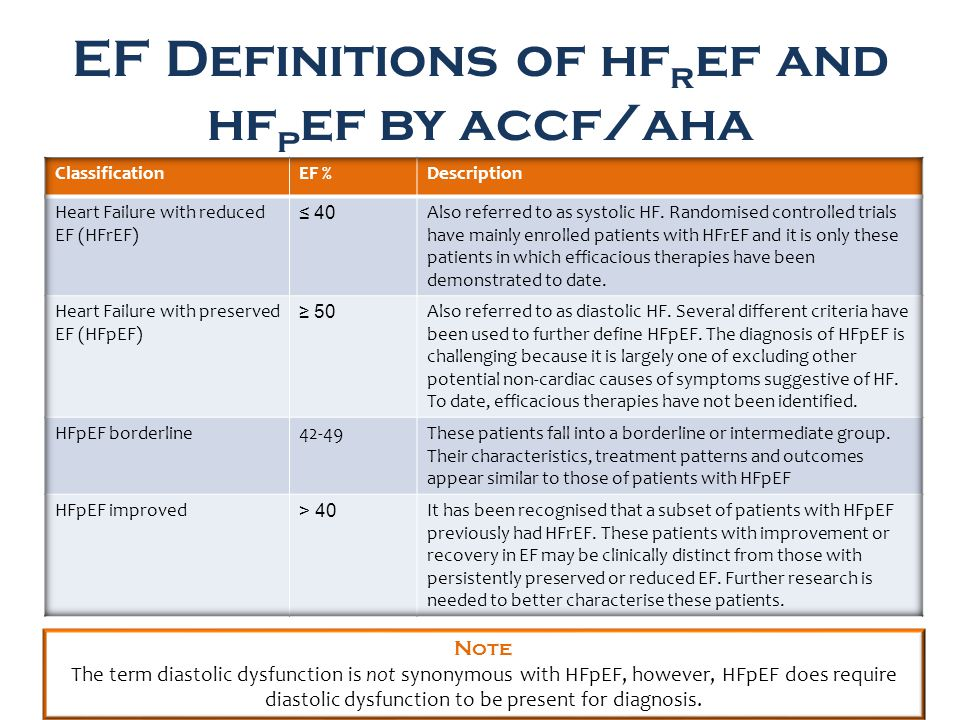
ESC criteria:

Pathophysiology underlying HFpEF
- many of the other pathological impairments noted in HFpEF are also seen in HFrEF and vice versa and we must ask whether HFpEF is a separate entity, a transition state into HFrEF or whether we are dealing with multiple different conditions where diastolic and systolic dysfunction are reflections of the underlying disease process
- key area to consider in the pathogenesis is the response to exercise
- a ventricle which may appear entirely normal at rest can respond abnormally when the patient is asked to exercise, with chronotropic impairment, diastolic changes or even frank systolic dysfunction occurring at higher heart ratess
- also consider changes in other body systems which place additional load upon the heart and cause contractile dysfunction owing to chronic changes in loading
Reference:
- Dunlay, S.M., V.L. Roger, and M.M. Redfield, Epidemiology of heart failure with preserved ejection fraction. Nat Rev Cardiol, 2017. 14(10): p. 591-602.
- Yancy, C.W., et al., 2013 ACCF/AHA Guideline for the Management of Heart Failure A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology, 2013. 62(16): p. E147-E239